Tobacco use is a leading contributor to death and disease, in Australia and internationally. Up to two-thirds of deaths in people who currently smoke can be attributed to smoking, who lose on average a decade of life.1 Smoking increases the risk of dying from many types of cancer, and several respiratory and cardiovascular diseases.2-4
It should be noted that the findings presented in this section vary between studies. This is largely due to differences in the methods used, the period of data collection, the age group of the study cohort, as well as variations in how diseases are classified or defined.5
3.30.1 Contemporary estimates of smoking attributable deaths
Epidemiological studies have been published that provide estimates of the burden of death and disease attributable to tobacco use in Australia.1,6 A major study investigating the mortality associated with smoking among Australians aged 45 years and over, found that smoking kills more than 24,000 people each year, equating to approximately 66 deaths per day. Smoking (current or past) was estimated to be responsible for 15.3% of deaths among Australians aged 45 years and over in 2019. The percentage of deaths differed between genders, with 19.4% of deaths in men and 11.1% of deaths in women attributed to smoking in 2019.6 Figure 3.30.1 and Table 3.30.1 present the number of deaths attributable to smoking among Australian men and women aged 45 years and over in 2019, by age group and by disease type.

3.30.2 The Australian Burden of Disease Study
Burden of disease research examines the overall effect of an illness on a population. This is typically achieved by determining the years of life and healthy life lost from diseases, injuries, and risk factors such as tobacco use. There are three commonly used burden of disease measures: disability-adjusted life years (DALYs), years of life lost (YLLs), and years lived with disability (YLDs). Table 3.30.2 presents these measures and their respective definitions as provided by the Australian Institute of Health and Welfare.2

The Australian Burden of Disease Study estimates the burden of more than 200 diseases and injuries, and 20 individual risk factors. The latest iteration of this study estimated that tobacco use contributed to 7.6% of the total disease burden in 2024. Since 2003, the total disease burden attributable to tobacco use has substantially decreased (by 41%) and it was found to be the second leading risk factor contributing to the total disease burden in 2024, behind overweight/obesity.2 Due in part to the comprehensive tobacco control measures implemented in Australia, this marks the first time that tobacco use was not the leading risk factor contributing to the total disease burden.
However, tobacco use remained the leading risk factor contributing to the fatal disease burden, with the Australian Burden of Disease Study estimating that it was responsible for 11.7% of the years of life lost in 2024.2
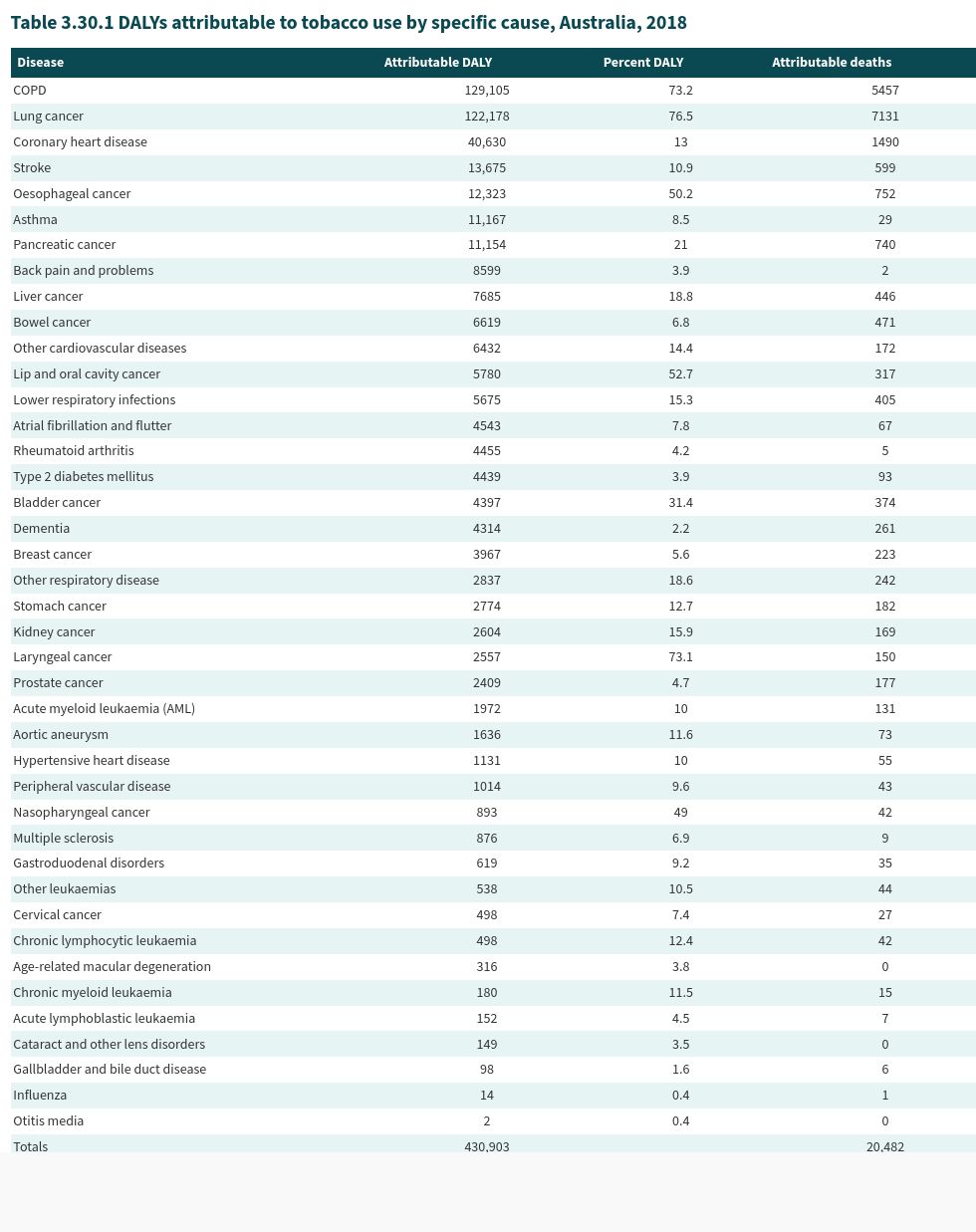
Tobacco use was linked to the burden of 41 diseases including 19 types of cancer, 7 cardiovascular diseases, and 4 respiratory diseases.2 Figure 3.30.2 sets out the total burden of disease attributable to tobacco use by disease group. It should be noted that the estimates provided in this figure differ to those displayed in Table 3.30.3 because of the proportional scaling that is applied to account for interactions between risk factors.

As demonstrated in Table 3.30.3, approximately 70% of the total disease burden from lung cancer, chronic obstructive pulmonary disease, and laryngeal cancer was attributable to tobacco use in 2024.

3.30.3 The Global Burden of Disease Study
The Global Burden of Disease Study is a large observational study examining levels and trends in death and disease burden across the world. It is designed to provide a global overview of disease burden and enable comparisons between countries.5 The latest (2021) iteration of this study estimated the burden of 371 diseases and injuries, and 88 different behavioural, environmental and occupational, and metabolic risk factors, across 204 countries and territories.7
Globally, there were an estimated 6.18 million (9.1%) deaths attributable to smoking in 2021. Compared to 2010, this is a 9.5% decrease. The percentage of deaths attributable to smoking in 2021 was different between genders, with 13.9% of male deaths and 3.1% of female deaths attributable to smoking.8
In addition, the percentage of deaths attributable to smoking differed between regions. In 2021, the World Health Organization Region with the highest percentage of deaths attributable to smoking was the Western Pacific Region (17.06%) followed by the European Region (8.98%), the South-East Asia Region (7.93%), the Region of the Americas (6.81%), the Eastern Mediterranean Region (6.12%), and the African Region (1.79%).4 Differences were also observed across socio-demographic (SDI) rankings. In 2021, high-middle SDI countries had the highest percentage of deaths attributable to smoking (13.02%) followed by middle SDI countries (10.58%), high SDI countries (10.06%), low-middle SDI countries (7.04%), and low SDI countries (2.67%).4
The Global Burden of Disease Study also provides estimates for the burden of disease attributable to chewing tobacco and secondhand smoke. It was estimated that 56,800 deaths and 1.5 million disability adjusted life years were attributable to chewing tobacco in 2021, with the majority of these occurring in South Asia.9 See Section 18A.3 for more information on the health effects of the different types of smokeless tobacco. Moreover, it was estimated that 1.29 million deaths and 34.9 million disability adjusted life years were attributable to secondhand smoke in 2021, with the 10.1% of the burden observed among children under the age of 5 years.10 See Section 4.7 for a discussion of the estimates of morbidity and mortality attributable to secondhand smoke.
For estimates of burden of disease in Australia it is preferrable to use the Australian Burden of Disease Study as it considers a greater number of factors compared to the Global Burden of Disease Study.
Related reading
Relevant news and research
A comprehensive compilation of news items and research published on this topic (Last updated December 2024)
Read more on this topic
Test your knowledge

References
1. Banks E, Joshy G, Weber MF, Liu B, Grenfell R, et al. Tobacco smoking and all-cause mortality in a large Australian cohort study: findings from a mature epidemic with current low smoking prevalence. BMC Medicine, 2015; 13(1):38. Available from: https://www.ncbi.nlm.nih.gov/pubmed/25857449
2. Australian Institute of Health and Welfare. Australian Burden of Disease Study 2024. Canberra AIHW. 2024. Available from: https://www.aihw.gov.au/reports/burden-of-disease/australian-burden-of-disease-study-2024.
3. Banks E, Joshy G, Korda RJ, Stavreski B, Soga K, et al. Tobacco smoking and risk of 36 cardiovascular disease subtypes: fatal and non-fatal outcomes in a large prospective Australian study. BMC Medicine, 2019; 17(1):128. Available from: https://www.ncbi.nlm.nih.gov/pubmed/31266500
4. Institute for Health Metrics and Evaluation (IHME). GBD Results. Seattle, USA: University of Washington, 2024. Available from: https://vizhub.healthdata.org/gbd-results/.
5. Zhao C, Choi C, Laws P, Gourley M, Dobson A, et al. Value of a national burden-of-disease study: a comparison of estimates between the Australian Burden of Disease Study 2015 and the Global Burden of Disease Study 2017. International Journal of Epidemiology, 2022; 51(2):668-78. Available from: https://pubmed.ncbi.nlm.nih.gov/34058000/
6. Joshy G, Soga K, Thurber KA, Egger S, Weber MF, et al. Relationship of tobacco smoking to cause-specific mortality: contemporary estimates from Australia. BMC Medicine, 2025; 23(1):115. Available from: https://pubmed.ncbi.nlm.nih.gov/39994694/
7. Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2021 (GBD 2021). Seattle, United States: Institute of Health Metrics and Evaluation, 2024. Available from: https://www.healthdata.org/research-analysis/gbd.
8. Institute for Health Metrics and Evaluation (IHME). GBD 2021 Cause and Risk Summary: Smoking. Seattle, USA University of Washington. 2024. Available from: https://www.healthdata.org/research-analysis/diseases-injuries-risks/factsheets/2021-smoking-level-3-risk.
9. Institute for Health Metrics and Evaluation (IHME). GBD 2021 Cause and Risk Summary: Chewing tobacco. Seattle, USA University of Washington. 2024. Available from: https://www.healthdata.org/research-analysis/diseases-injuries-risks/factsheets/2021-chewing-tobacco-level-3-risk.
10. Institute for Health Metrics and Evaluation (IHME). GBD 2021 Cause and Risk Summary: Secondhand smoke. Seattle, USA University of Washington. 2024. Available from: https://www.healthdata.org/research-analysis/diseases-injuries-risks/factsheets/2021-secondhand-smoke-level-3-risk.